




Pharmacovigilance is frequently reduced to a reporting exercise. Meet the deadline, submit the case, move on. That framing is not just incomplete. It actively creates compliance risk. The real role of pharmacovigilance in compliance spans the entire product lifecycle, touching signal detection, risk management planning, quality system design, and regulatory inspection readiness. This guide breaks down each dimension clearly, so regulatory affairs professionals and compliance officers can build programs that satisfy regulators and protect patients, not just check boxes on a submission calendar.
Table of Contents
- Key takeaways
- Role of pharmacovigilance in compliance frameworks
- Pharmacovigilance systems as quality frameworks
- Lifecycle risk management and signal detection
- Practical compliance pitfalls in PV operations
- Demonstrating PV compliance effectiveness in 2026
- My perspective on building real PV compliance
- Strengthen your pharmacovigilance compliance program
- FAQ
Key takeaways
| Point | Details |
|---|---|
| PV compliance is system-wide | Regulators assess your entire pharmacovigilance quality system, not just individual case submissions. |
| Timelines are table stakes | Serious adverse reactions must be reported within 15 days; meeting that baseline is mandatory but not sufficient. |
| Signal detection links to action | Identifying a safety signal only counts as compliance when it connects to documented risk minimization decisions. |
| Audit trails must be traceable | Every handoff from initial signal awareness through final submission must be documented with verifiable timestamps. |
| Effectiveness evidence is the new standard | EMA’s 2026 pilot signals that inspectors now evaluate whether quality systems actually work, not just whether SOPs exist. |
Role of pharmacovigilance in compliance frameworks
Most regulatory professionals understand pharmacovigilance as the science and operational system for monitoring, detecting, and preventing adverse drug reactions. WHO frames pharmacovigilance as a compliance obligation built into the product lifecycle, not an optional monitoring layer. That framing matters for how you structure your program.
Global regulatory frameworks each define specific pharmacovigilance compliance obligations, and they do not always align neatly:
- EMA GVP Modules: The Good Pharmacovigilance Practices guidelines govern Individual Case Safety Reports (ICSRs), Periodic Benefit-Risk Evaluation Reports (PBRERs), signal management, risk management plans, and the Pharmacovigilance System Master File (PSMF).
- FDA regulations: 21 CFR Part 314 and Part 600 govern post-market safety reporting, including expedited and periodic reporting requirements for approved drugs and biologics.
- WHO guidelines: Provide harmonized standards for countries outside the EU and US regulatory zones, shaping expectations in emerging markets where your products may also be distributed.
- ICH guidelines: Specifically E2A through E2F, these cover definitions, data elements, and workflows for safety reporting across jurisdictions.
The Qualified Person for Pharmacovigilance (QPPV) sits at the center of this structure. The QPPV is responsible for the pharmacovigilance system overview and must have continuous access to the PSMF, safety information, and records of all decisions made within the system. Compliance is not possible if the QPPV role is filled on paper only. Correct data elements with verifiable timestamps are what EMA uses to calculate compliance, which means every intake source, every handoff, and every submission must generate reliable metadata.
For regulatory compliance in pharmacovigilance, the distinction between serious and non-serious ICSRs is foundational. Serious adverse reactions carry a 15-day reporting deadline to EudraVigilance. Non-serious cases carry a 90-day window. Missing either consistently will trigger compliance notifications from EMA and place your organization on a watch list that informs inspection scheduling.
Pharmacovigilance systems as quality frameworks
Moving from individual case management to system-level thinking is where most organizations either gain or lose ground with regulators. Regulators evaluate the systems behind submissions, not just the individual cases, which requires comprehensive quality-system documentation at every layer.
A well-designed pharmacovigilance quality system typically includes these core components:
- Standard Operating Procedures (SOPs): Written, version-controlled, and actively trained. SOPs must cover case intake, triage, seriousness assessment, medical review, data entry, quality check, and final submission.
- Training records: Personnel must have documented training against current SOP versions. Regulators want evidence that training happened before the person worked cases, not after a deviation.
- Audit trails: All systems used for case processing must generate immutable logs showing who did what, when, and what was changed.
- Deviation management: Every missed timeline, data error, or process failure must be captured, investigated, and linked to corrective action.
- CAPA program: Corrective and preventive actions must close within agreed timeframes, with documented evidence that the fix actually worked.
- Vendor and affiliate oversight: Contract research organizations, local affiliates, and licensed partners must operate under binding pharmacovigilance agreements that define responsibilities, timelines, and escalation paths.
The Pharmacovigilance System Master File ties all of this together. It must describe your organization’s system, the QPPV’s oversight role, the database infrastructure, and the contracted service relationships. Inspectors will request the PSMF on day one. If it does not accurately reflect your actual operations, every discrepancy becomes a finding.
Pro Tip: Before any scheduled inspection, conduct a structured walkthrough of your PSMF against your actual case processing workflow. Discrepancies found internally are correctable. Discrepancies found by an inspector are findings.
Evaluating pharmacovigilance due diligence requires reviewing operational capabilities including validated safety databases, qualified personnel, SOP maintenance, and historical inspection outcomes. This same lens applies to any vendor or affiliate whose activities your organization is legally responsible for.
Lifecycle risk management and signal detection
Pharmacovigilance compliance strategies cannot be limited to post-market case processing. The ICH E2E guideline on pharmacovigilance planning requires documented safety specifications and signal workflows beginning at the development stage, before your product reaches patients at scale.
Understanding where risk management fits across the lifecycle helps clarify compliance obligations at each stage:
| Document | When required | Compliance function |
|---|---|---|
| Pharmacovigilance Plan | Pre-authorization, updated post-launch | Documents monitoring commitments for identified and potential risks |
| Risk Management Plan (RMP) | Required by EMA for new marketing authorizations | Specifies risk minimization measures and success metrics |
| PBRER | Periodically throughout product lifecycle | Integrates benefit-risk balance with safety signal analysis |
| PSMF | Maintained continuously post-authorization | Serves as master reference for PV system inspection readiness |
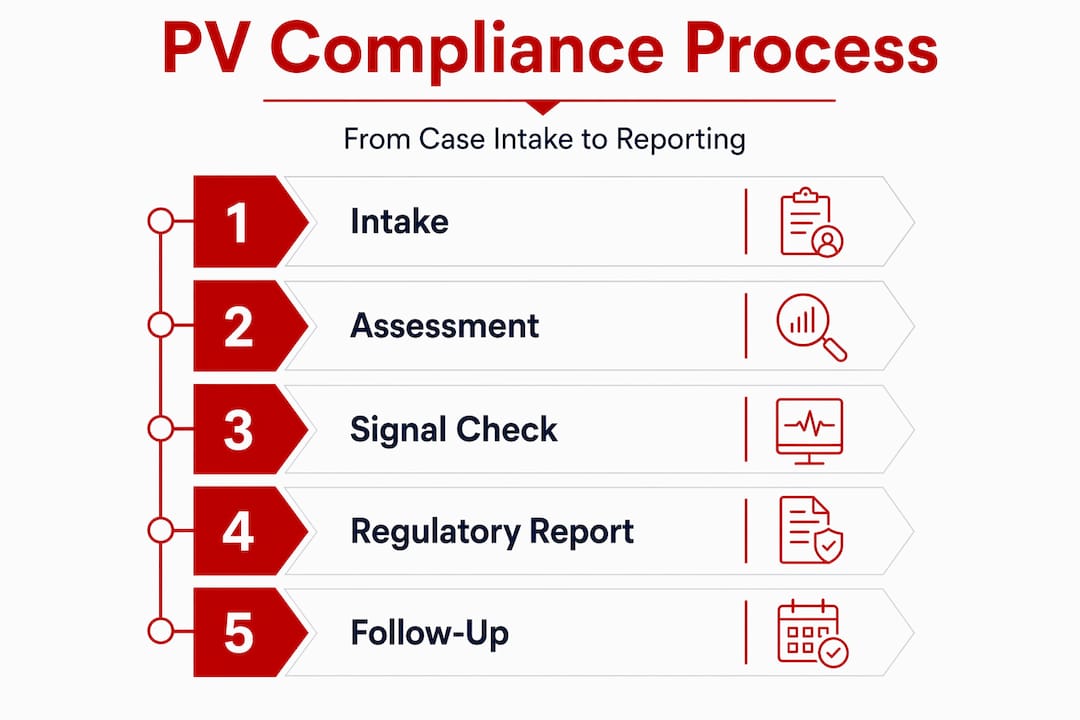
Signal detection is where the importance of pharmacovigilance becomes most visible to regulators. The process moves through four stages: identification, validation, assessment, and recommendation. Identification happens through aggregate case review, literature monitoring, and data mining from EudraVigilance or FDA Adverse Event Reporting System. Validation confirms the signal is based on sufficient evidence to warrant further assessment. Assessment weighs causality, severity, and frequency. Recommendation produces a regulatory action, whether that is a label update, a Dear Healthcare Professional communication, or a formal risk minimization measure.

The compliance gap that many organizations miss is that signal detection findings must connect to documented regulatory decisions. Finding a signal and not documenting the subsequent risk assessment and management decision creates a serious compliance vulnerability. WHO’s framing of PV as preventive safety science reinforces this point: compliance activities must connect reporting obligations to genuine risk minimization, not just close the detection loop on paper.
For those building or refining their signal detection capabilities, the pharmacovigilance signal detection services available through Jjccgroup provide a practical consulting framework for mapping these workflows to your existing quality infrastructure.
Practical compliance pitfalls in PV operations
Knowing the requirements is one thing. Operationalizing them across a global organization, multiple vendors, and changing affiliate structures is where compliance failures actually occur. Common pitfalls include unclear day-zero determination, inconsistent affiliate training, and missing documentation of key decisions.
The most consequential challenges compliance officers encounter include:
- Day-zero ambiguity: Day zero in pharmacovigilance is the date the company first became aware of a case meeting minimum reportability criteria. When multiple intake channels exist, including medical information, social media, clinical trials, and affiliate networks, determining which awareness event starts the clock is operationally complex and must be defined explicitly in SOPs.
- Data quality failures: Incomplete cases with missing patient identifiers, suspect drug information, or adverse event descriptions create downstream compliance exposure. EMA calculates compliance based on the completeness and accuracy of submitted data elements, not just submission dates.
- Vendor agreement gaps: Pharmacovigilance agreements with contract organizations must specify data exchange timelines, quality expectations, and escalation procedures. Vague language around “timely reporting” without defined hour and day thresholds will not survive inspection scrutiny.
- System-focused versus case-focused compliance: Treating PV compliance as case-focused leads to neglect of the end-to-end quality system regulators actually evaluate, including SOP control, training, and audit trails.
Pro Tip: Map your intake sources annually and document the day-zero decision logic for each source in a dedicated SOP. Auditors will specifically test whether your day-zero rules match the actual case timestamps in your safety database.
Inspection preparation requires selecting a representative sample of cases from diverse intake sources and verifying every documented step: intake, triage, seriousness assessment, medical review, follow-up requests, and final submission. Demonstrating traceability across different intake sources is what separates a compliant organization from one that simply processes cases competently.
Demonstrating PV compliance effectiveness in 2026
Regulatory expectations are shifting in a meaningful direction. EMA’s 2026 to 2027 pharmaceutical quality system effectiveness pilot assesses how organizations can demonstrate that risk-based change management actually works, not just that it is documented. This is a significant change in inspection philosophy.
The practical implications for pharmacovigilance compliance programs are concrete:
| Compliance area | Documentation standard (pre-2026) | Effectiveness evidence (2026 and beyond) |
|---|---|---|
| CAPA program | Closed CAPAs with documented actions | Evidence that the corrective action resolved the root cause |
| Training program | Attendance records and completion logs | Pre/post assessment results, error rate trends in trained staff |
| Deviation management | Deviations logged and categorized | Trend analysis showing reduction in repeat deviations |
| Management review | Meetings held with minutes | Decisions made, actions taken, and outcomes documented |
PV compliance is increasingly judged by effectiveness evidence, not just adherence to written procedures. Organizations that design their quality systems around demonstrable outcomes will be far better positioned than those maintaining document libraries that describe processes no one can verify actually work.
The PIC/S guidance referenced in EMA’s pilot reinforces risk-based approaches throughout. This means your change control process, your CAPA closure standards, and your management review agenda should all be structured around risk tiering. Not every deviation requires the same level of investigation. But every deviation does require documented evidence that its resolution matched the risk it represented.
Understanding how these expectations translate to FDA-specific compliance contexts is where resources like FDA compliance strategy guidance from Jjccgroup become useful reference points for building your internal program.
My perspective on building real PV compliance
I have reviewed pharmacovigilance programs across a range of organizational sizes, and the pattern is consistent. Organizations that struggle with inspections are rarely ignorant of the regulations. They have SOPs. They have a QPPV. They submit cases. The problem is that their compliance program is built around activities rather than outcomes.
When I see a deviation log that was never connected to a CAPA, or a vendor agreement that defines timelines in vague terms, or a training program that generates certificates but no evidence of competency, I know what an inspector is going to find before they find it.
The organizations that consistently pass inspections are the ones that treat pharmacovigilance as a risk management discipline, not a reporting service. They assign ownership to system components, not just case queues. They conduct pre-inspection simulations with real case samples pulled from their actual intake sources. They can tell you their compliance rate by source channel, not just overall.
What I would encourage every compliance officer to do right now is pull five cases from different intake sources and trace the documentation from awareness to submission yourself. Not a quality auditor. You, personally. What you find in that exercise will tell you more about your program’s actual compliance posture than any SOP walkthrough or dashboard review.
Proactive regulatory intelligence also matters here. The EMA’s 2026 effectiveness pilot is not a distant future concern. Inspectors are already applying this lens. Getting ahead of it requires designing your metrics and management review outputs today, not after your first critical finding.
— Mike
Strengthen your pharmacovigilance compliance program
For organizations that recognize the gap between documentation and demonstrated effectiveness, Jjccgroup’s regulatory consulting team works directly with pharmaceutical and medical device companies to build pharmacovigilance systems that hold up under inspection.
With over 30 years of experience in FDA regulatory compliance, Jjccgroup provides gap assessments against current GVP and FDA expectations, system design support for quality-system components, audit preparation services, and targeted training programs for PV operations teams. Whether you are preparing for a routine inspection, responding to a compliance notification, or building a new pharmacovigilance system from the ground up, the team at Jjccgroup has the operational depth to support your program. Explore FDA regulatory compliance consulting or review the pharmaceutical compliance consulting guide to identify where your program needs the most attention.
FAQ
What is the role of pharmacovigilance in compliance?
Pharmacovigilance supports regulatory compliance by providing the systems, documentation, and processes that regulators use to verify product safety is being actively managed throughout the product lifecycle. It covers case reporting, signal detection, risk management planning, and quality system oversight.
How does pharmacovigilance ensure compliance with reporting timelines?
EMA requires serious adverse reactions to be submitted within 15 days and non-serious cases within 90 days, with compliance calculated from verifiable timestamps in electronic case reports. Accurate day-zero determination and data completeness are as critical as meeting the deadline itself.
What are the most common pharmacovigilance compliance failures?
The most frequent failures involve unclear day-zero rules, incomplete case data, vague vendor agreements, and a case-focused approach that neglects the broader quality system requirements regulators actually inspect.
How is pharmacovigilance compliance changing in 2026?
EMA’s 2026 to 2027 pharmaceutical quality system effectiveness pilot shifts inspection focus from documentation alone to evidence that quality systems actually produce intended outcomes, requiring organizations to design metrics, management reviews, and CAPA programs that demonstrate real-world effectiveness.
What is the PSMF and why does it matter for compliance?
The Pharmacovigilance System Master File is the master reference document describing your organization’s pharmacovigilance system. Inspectors request it on day one of any inspection, and discrepancies between its contents and actual operations immediately become findings.
Recommended
- 5 Best Pharmacovigilance Remote Courses for 2025 – J&J Consulting Group- FDA Regulatory Compliance
- A Guide to Pharmacovigilance Signal Detection Services
- Pharmaceutical Compliance Consulting: Your Guide to FDA Approval – J&J Consulting Group- FDA Regulatory Compliance
- Your Guide to Pharmaceutical Regulatory Consulting – J&J Consulting Group- FDA Regulatory Compliance