




Design controls in medical devices are the regulatory-mandated procedures and practices manufacturers must implement to confirm their devices meet specified design requirements and user needs before market release. Under 21 CFR 820.30, the FDA requires these controls as a structured system governing the entire design lifecycle, from the first definition of user needs through to design transfer and post-market changes. ISO 13485:2016 Clause 7.3 mirrors these requirements internationally, making design controls the common language of device quality across global regulatory submissions. For regulatory affairs professionals and quality assurance managers, understanding this framework is not optional. It is the foundation of every compliant product development program.
What are design controls in medical device development?
Design controls are a system of interrelated procedures forming checks and balances that govern the complete design lifecycle, not just isolated documents or project phases. The FDA’s 1997 Design Controls Guidance frames them as a continuous process running from the initial capture of user needs through design transfer to manufacturing. This means every decision made during development must be documented, traceable, and defensible against regulatory scrutiny.
The importance of design controls extends beyond audit readiness. They exist because device failures frequently trace back to inadequate design processes rather than manufacturing defects. A device built exactly to its specifications can still harm patients if those specifications were never properly derived from real user needs. Design controls close that gap by requiring manufacturers to prove both that the design was executed correctly and that the right design was chosen in the first place.
Class II and Class III devices are subject to full design control requirements under 21 CFR 820.30. Most Class I devices are exempt, but software-driven Class I devices and those with specific risk profiles may still fall under the rule. Regulatory affairs teams should confirm applicability early in the product development program, since retrofitting design controls onto a completed project is one of the most expensive mistakes in device development.
What are the key design control requirements under FDA and ISO standards?
The FDA specifies 10 core elements under 21 CFR 820.30 that together constitute a complete design control system. Each element is distinct but feeds directly into the next, creating a traceable chain of evidence from user need to finished device.
- Design and development planning: A written plan defining phases, responsibilities, and review points throughout development.
- Design inputs: Documented physical, performance, safety, and regulatory requirements that the device must satisfy.
- Design outputs: Specifications, drawings, software code, and manufacturing procedures that translate inputs into a buildable product.
- Design reviews: Formal, documented evaluations at defined stages, conducted by personnel not directly responsible for the design work under review.
- Design verification: Testing and analysis confirming that outputs meet inputs.
- Design validation: Testing confirming the finished device meets user needs under actual or simulated use conditions.
- Design transfer: The controlled process of moving the validated design into full-scale production.
- Design changes: A formal change control process covering all modifications after design freeze, including post-market changes.
- Design History File (DHF): The master record demonstrating that the design was developed in accordance with the approved plan.
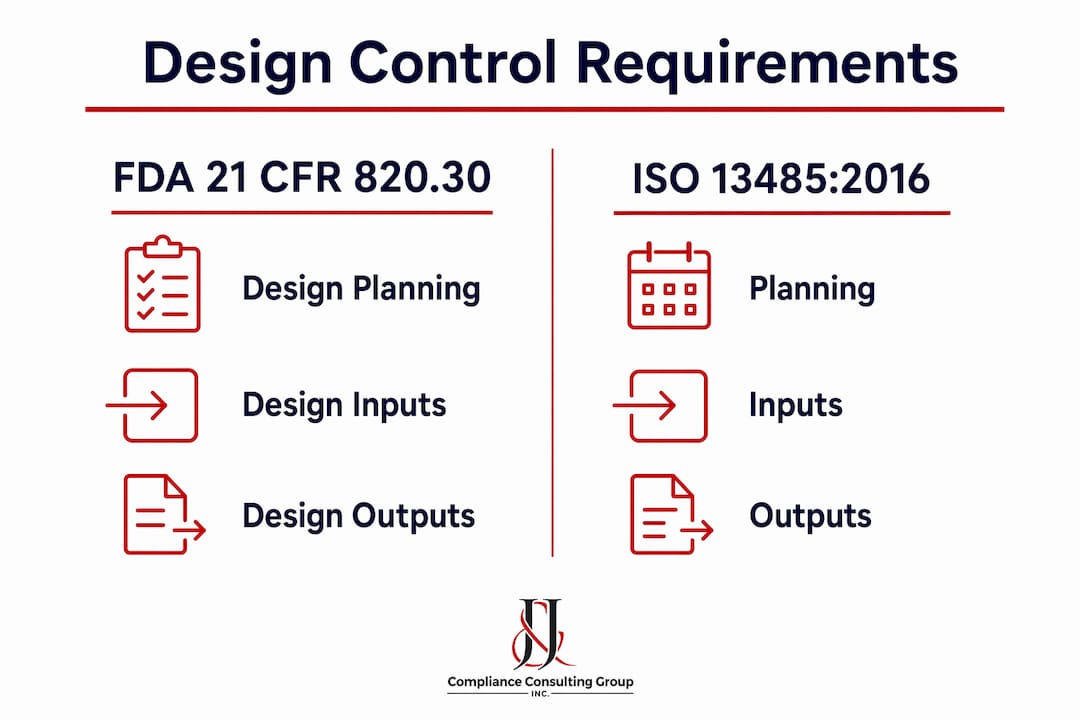
ISO 13485:2016 Clause 7.3 aligns closely with these FDA elements, covering planning, inputs, outputs, reviews, verification, validation, transfer, and change control within a unified quality management system framework. The practical difference is that ISO 13485 applies globally and is the basis for CE marking in the European Union, while 21 CFR 820.30 governs FDA-regulated markets. Under the FDA’s new Quality Management System Regulation (QMSR), which took effect in February 2026, the agency formally harmonized its requirements with ISO 13485, reducing the compliance burden for manufacturers operating in both markets.
| Requirement area | FDA 21 CFR 820.30 | ISO 13485:2016 Clause 7.3 |
|---|---|---|
| Design planning | Required, written plan | Required, documented plan |
| Design inputs and outputs | Explicitly required | Explicitly required |
| Verification and validation | Separate activities required | Separate activities required |
| Design History File | Required | Technical file equivalent |
| Change control | Formal process required | Formal process required |
Documentation and traceability expectations run through every element. The DHF must demonstrate that each output traces back to a specific input, that verification tested the right outputs, and that validation covered the intended use population. Gaps in this chain are among the most common findings in FDA inspections.
How do design verification and validation differ in practice?
Design verification answers the question: “Did we build the device right?” It confirms that design outputs meet design inputs through testing, inspection, and analysis conducted against documented acceptance criteria. Verification happens on prototypes or production-equivalent units and does not require end users to be involved.
Design validation answers a different question entirely: “Did we build the right device?” Validation confirms that the finished device, in its final production form, meets the needs of the intended user population under actual or simulated use conditions. This distinction matters because a device can pass every verification test and still fail in clinical use if the original design inputs were incomplete or incorrect.
Common verification methods include dimensional inspection, electrical safety testing per IEC 60601, biocompatibility testing per ISO 10993, and software unit testing. Validation methods typically include simulated use studies, human factors validation testing per FDA’s 2016 Human Factors Guidance, and clinical evaluations. Both activities require formal protocols written before testing begins, with acceptance criteria defined in advance rather than after reviewing results.
Pro Tip: Write verification and validation protocols before generating any test data. Protocols written after the fact, even when the data is legitimate, create the appearance of post-hoc rationalization and are a consistent target during FDA inspections.
The most common pitfall is treating validation as an extension of verification rather than a separate activity with its own evidence requirements. Regulatory submissions that blur this line, such as submitting bench test data as evidence of validation, draw immediate scrutiny from FDA reviewers. Maintaining separate protocol numbers, separate reports, and separate traceability entries in the DHF keeps the distinction clear and defensible.
What are the practical challenges in implementing design controls?
Traceability is the single most persistent challenge in design control implementation. The DHF must demonstrate that every design input is addressed by at least one output, that every output has been verified, and that validation covers the full scope of intended use. In practice, most teams manage this through a Design Traceability Matrix (DTM), which maps inputs to outputs to verification to validation in a single navigable document. Without a DTM, auditors spend hours reconstructing linkages that should be immediately apparent, and gaps become visible only under pressure.
Lifecycle integration presents a second layer of complexity. Design controls do not end at design transfer. Post-market design changes, whether driven by CAPA findings, complaint trends, or manufacturing process updates, require the same formal change control process as pre-market modifications. Teams that treat design controls as a pre-market activity consistently struggle when FDA inspectors ask for evidence that post-market changes were evaluated for impact on validation status.
Software medical devices introduce additional requirements. Software design outputs must include architecture documents, software requirements specifications, code review records, and traceability matrices linking software requirements to test cases. The FDA’s guidance on Software as a Medical Device (SaMD) and IEC 62304 both require that software verification and validation be protocol-driven, with acceptance criteria defined at the unit, integration, and system levels. Agile development teams often find this challenging because iterative sprints do not map cleanly onto the linear phase structure implied by 21 CFR 820.30.
Best practices that consistently reduce audit risk include the following:
- Assign a dedicated design control coordinator who owns the DHF and traceability matrix throughout the project.
- Conduct design reviews with cross-functional participation, including representatives from regulatory affairs, quality, manufacturing, and clinical or human factors.
- Use electronic quality management system (eQMS) platforms such as Veeva Vault QMS, MasterControl, or Greenlight Guru to maintain living traceability rather than static spreadsheets.
- Document design change rationale explicitly, including the impact assessment on existing verification and validation evidence.
How do design controls fit into the broader quality management system?
Design controls do not operate in isolation. Under the new QMSR framework, FDA inspectors expect design controls to be visibly linked to risk management, CAPA, complaint handling, and post-market surveillance. A CAPA opened in response to a field complaint, for example, may require a formal design change, which in turn triggers a re-verification or re-validation activity. That chain of evidence must be traceable across subsystems, not siloed within individual departments.
Risk management under ISO 14971:2019 is the most direct integration point. Design inputs must reflect risk control measures identified during hazard analysis, and design validation must confirm that those controls are effective in actual use. Manufacturers that treat risk management as a separate document exercise, disconnected from the design input and validation records, create a compliance gap that is difficult to close retroactively.
The following sequence illustrates how design controls connect to the broader QMS during a typical product lifecycle:
- User needs and intended use are defined, triggering a risk management plan under ISO 14971.
- Design inputs are derived from user needs and risk control requirements.
- Design outputs are developed and verified against inputs.
- Design validation confirms user need satisfaction and risk control effectiveness.
- Design transfer moves the validated design to manufacturing with documented acceptance criteria.
- Post-market surveillance data feeds back into the risk management file and may trigger design changes through the CAPA system.
Premarket submissions to the FDA, including 510(k) notifications and PMA applications, require evidence that design controls were followed. Reviewers examine design inputs, verification and validation summaries, and risk management reports as part of the substantial equivalence or safety and effectiveness determination. A well-maintained DHF makes this evidence readily accessible and reduces the likelihood of additional information requests that delay clearance or approval.
Key takeaways
Design controls are the structured, traceable framework that connects user needs to a validated, market-ready device, and their integration with risk management, CAPA, and post-market surveillance is what separates compliant manufacturers from those who face repeated FDA findings.
| Point | Details |
|---|---|
| Regulatory basis | 21 CFR 820.30 and ISO 13485:2016 Clause 7.3 define the required design control elements. |
| Verification vs. validation | Verification confirms outputs meet inputs; validation confirms the device meets real user needs. |
| DHF traceability | A navigable Design Traceability Matrix linking inputs, outputs, verification, and validation is the core audit defense. |
| Lifecycle obligation | Design controls apply post-market; every change requires formal impact assessment and documented rationale. |
| QMS integration | Risk management under ISO 14971, CAPA, and post-market surveillance must link visibly to design control records. |
What I’ve learned after decades of design control reviews
After working through hundreds of design control audits and submissions across device classes, the pattern I see most often is not ignorance of the requirements. Most regulatory and quality professionals know what 21 CFR 820.30 says. The failure point is almost always execution at the traceability level. Teams build a DHF that looks complete on the surface but falls apart the moment an auditor asks a simple question: “Show me where this design input is validated.” If that question takes more than two minutes to answer, the system has a problem.
The shift toward QMSR compliance has raised the stakes further. Transitioning from legacy inspection models to a process-based framework requires interconnected documentation that crosses departmental boundaries. I have seen companies with excellent individual procedures fail inspections because no one owned the connections between those procedures. Design controls, risk management, and CAPA need to speak the same language, reference the same document numbers, and tell a coherent story about how the device was developed and how it is maintained.
The software device space is where I see the most creative tension right now. Agile teams resist the documentation overhead of formal design controls, and that resistance is understandable. But the answer is not to abandon structure. It is to build lightweight, traceable artifacts at each sprint that accumulate into a defensible DHF. Companies that solve this problem gain a real competitive advantage in submission timelines.
— Mike
Work with Jjccgroup on your design control program
Jjccgroup brings over 30 years of FDA and ISO regulatory expertise to medical device manufacturers who need more than a checklist. Whether you are building a design control system from the ground up, preparing for an FDA inspection, or aligning an existing QMS with the new QMSR requirements, Jjccgroup provides the hands-on consulting support that turns regulatory obligation into a competitive asset.
From design control implementation and DHF gap assessments to software as a medical device compliance and premarket submission support, Jjccgroup’s team works alongside your regulatory and quality functions as a true partner. Explore Jjccgroup’s FDA compliance consulting services to see how a structured, audit-ready design control program can accelerate your path to market.
FAQ
What is design controls in medical device regulation?
Design controls are the FDA-required system of procedures under 21 CFR 820.30 that manufacturers must follow to confirm a device meets its design requirements and user needs throughout development. ISO 13485:2016 Clause 7.3 establishes equivalent requirements for international markets.
Which device classes must comply with design control requirements?
Class II and Class III devices are subject to full design control requirements under 21 CFR 820.30, while most Class I devices are exempt. Software-driven Class I devices and certain higher-risk Class I products may still require compliance.
What is the Design History File and why does it matter?
The Design History File is the comprehensive record demonstrating that a device was developed in accordance with the approved design plan. It serves as the primary evidence document during FDA inspections and premarket submissions.
How does design validation differ from design verification?
Verification confirms that design outputs meet design inputs, while validation confirms the finished device meets actual user needs under real or simulated use conditions. Both require formal protocols with pre-defined acceptance criteria.
Do design controls apply after a device is already on the market?
Yes. Any post-market design change requires formal change control under 21 CFR 820.30, including an impact assessment on existing verification and validation evidence and an updated DHF entry.